As technology continues to advance and more men and women are talking about their struggles with infertility, couples are becoming more proactive about their reproductive health and seeking the expertise of a fertility specialist. On average, it will take a couple 5-7 months to conceive, so there’s no need to become concerned if it’s taking you more than a few months to get pregnant. But as more time passes without success, how do you know when it’s time to seek help?
Physicians often suggest seeking a complete fertility evaluation after 12 months of trying to conceive with no success when the female partner is under the age of 35, after 6 months when she is older than 35, and after 3 months if 40 and over. Beyond age, it is important to be aware of several medical conditions that indicate seeing a fertility specialist sooner. If any of the following conditions apply to you, it is probably time to make an appointment with a fertility specialist:
1. YOUR PERIOD IS IRREGULAR OR SOMETIMES DOESN’T COME AT ALL
Irregular periods usually mean irregular ovulation and no periods at all may mean ovulation is not taking place, making conception feel like an uphill battle. While there are many reasons why you may miss your period, ovulatory disorders are the leading cause of infertility for women.
“Ovulatory disorders broadly break down into two groups: no ovulation and oligo-ovulation (frequently due to PCOS), which is when ovulation occurs infrequently or irregularly,” explains Dr. Bromer. Medications such as Clomid and treatment options such as intrauterine insemination (IUI) can induce ovulation and help patients conceive faster. No matter your age, if ovulation is irregular or never occurring, seeking the help of a specialist can help get your reproductive system back on track.
2. YOU HAVE BEEN TRYING…..BUT NOT REALLY….
“During initial consultations with patients, I have many who say, ‘We haven’t used any forms of contraception in the past three years, but we have only really been trying to conceive for about six months.’ So what does ‘trying’ really mean?” asks Dr. Jason Bromer. “No matter if you have been actively trying or not, couples having unprotected sexual intercourse for more than 6 or 12 months, depending on age, should seek a fertility evaluation if they are not conceiving.”
“We can order specialized testing to detect subtle causes of infertility,” says Dr. Bromer. Based on the information learned through testing, fertility specialists can offer several low-tech treatment options to start, which are often covered by insurance.
3. YOU HAVEN’T HAD A COMPREHENSIVE FERTILITY WORK-UP….AND TREATMENT HASN’T BEEN SUCCESSFUL YET
At Shady Grove Fertility, the very first thing your fertility specialist will do is review your medical history and initiate fertility testing for both partners. It is very important that each of the following tests be performed prior to initiating any kind of fertility treatment, because a complete evaluation of the male and female reproductive functions are required to determine the cause of infertility and identify the most effective course of treatment.
These basic tests include:
- Day 3 bloodwork: tells you if your reproductive hormones are functioning normally.
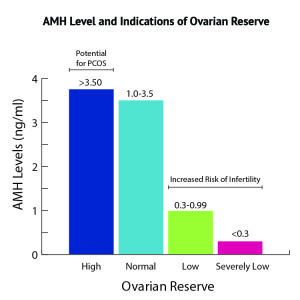
- Anti-Müllerian hormone (AMH) test: tells you how many eggs you have.
- Hysterosalpingogram (HSG): tells you if your uterus is shaped normally and if your tubes are open.
- Semen analysis: tells you if your partner has enough sperm and if they are healthy.
4. THE SEMEN ANALYSIS IN YOUR FERTILITY WORK-UP CAME BACK ABNORMAL
While often considered a female health concern, 40 percent of all infertility cases are in part due to male factor infertility. If you have received abnormal semen analysis results, you should see a fertility specialist right away. When the male partner’s sperm count is low or of poor quality, it can make conception significantly more difficult. Seeing a fertility specialist can help to determine the severity of a potential male factor diagnosis and offer a range of solutions to help you conceive. “The good news if you have a low sperm count is it only takes a single sperm to make a great embryo,” says Dr. Bromer. Modern reproductive technology like in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) can help patients with even the lowest sperm counts overcome infertility.
5. YOU HAVE EXPERIENCED TWO OR MORE MISCARRIAGES
It is a common misconception that women who have miscarriages are just fine because they are able to get pregnant. “In fact, having multiple miscarriages is a very specific type of fertility problem that affects 1-3 percent of all couples,” explains Dr. Bromer. “The majority of miscarriages can be attributed to genetic abnormalities in the embryo, while other causes include hormonal problems like diabetes, thyroid disease, undetected structural problems in the uterus, and advanced reproductive age.” Anyone who has experienced two or more miscarriages should see a fertility specialist.
IT’S TIME TO SEE A FERTILITY SPECIALIST
Making the move to see a fertility specialist is a big step for many people. Patients often second-guess themselves about the need to see a specialist, or they worry that it won’t work or how will they afford it. It’s best to take it one step at a time. By scheduling a new patient consultation–which is covered by insurance in 90% of cases–you will get the answers you need to help you move forward. Shady Grove Fertility’s specially trained reproductive endocrinologists are among the best in the field and are dedicated to working with each patient to overcome their infertility.

Medical Contribution by: Jason Bromer, M.D., of Shady Grove Fertility’s Frederick, MD office.
Early intervention offers the best chances of success, so let us help you get started. To learn more about our simple fertility evaluation or to schedule an appointment, please call our New Patient Center and one of our New Patient Liaisons will happily assist you. Please call 1-877-971-7755 or click to complete this simple form.
At Shady Grove Fertility, we’re here to give you the caring support you deserve as you start or grow your family. As a leading fertility and IVF center of excellence, we offer patients individualized care, innovative financial options, over 30 accepted insurance plans, and pregnancy rates among the highest of all national centers. We offer patients the convenience of 19 full-service and 6 satellite locations across Maryland, Pennsylvania, Virginia, and Washington, D.C. More than 1,700 physicians choose Shady Grove Fertility to refer their patients, and more than 96 percent of our patients say they would recommend Shady Grove Fertility’s 35+ physicians to a friend. With 10 Shady Grove Fertility babies born each day, your dream of starting or growing your family is within reach.