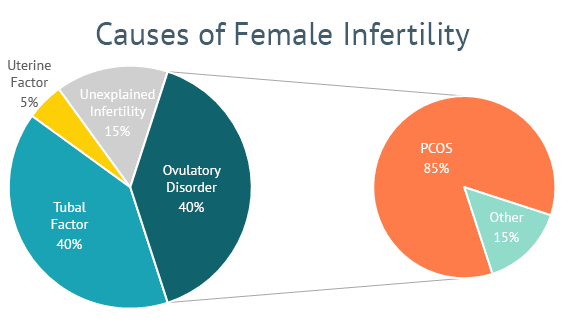
With nearly one-third of all infertility diagnoses in women, polycystic ovary syndrome, or PCOS, is the most common ovulatory disorder in women of reproductive age.
“While myths persist that women with PCOS cannot get pregnant, the reality is that it is highly treatable and nearly every woman with PCOS should be able to get pregnant,” explains Dr. Celso Silva, Shady Grove Fertility Tampa Bay Medical Director. “In fact, many women will experience increases in fertility through lifestyle changes and modest weight loss. Others will find success with basic infertility treatments and medications. And for those that need additional help conceiving, in vitro fertilization (IVF) is a highly effective form of treatment for women with PCOS.”
Medical contribution by Celso Silva, M.D.
Celso Silva, M.D., M.S., is board certified in obstetrics and gynecology and reproductive endocrinology and infertility. Dr. Silva sees patients at SGF’s Tampa – Westshore office.
What are the symptoms of PCOS?
PCOS affects approximately 5 to 10 percent of the population, and is most prevalent in Hispanics and African Americans. Recent studies also suggest that there is a rising rate in women of Asian descent.
Some of the most recognizable symptoms of PCOS include absent or irregular menstrual cycles, acne, and excessive body hair growth. While many people may consider obesity as a main symptom of the disease, approximately one-third of women with PCOS have normal weight or are underweight.
What causes PCOS?
Although the specific cause of PCOS is still unknown, the condition results in hormonal imbalances that curtail or prevent ovulation—the body’s process of producing and releasing eggs from the ovary. It is common for women with PCOS to have an inappropriate production of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). As a result, they experience limited follicular development (follicles are small sac-like structures within the ovaries, and each follicle contains an egg). With limited follicular development, egg development will not occur. Also as a result, women with PCOS have an increase in testosterone and other typically male hormones (androgens).
Clinically, the limited egg development may result in irregular ovulation or a complete lack of ovulation (anovulation), which can persist for months or even years. This ovulatory dysfunction is what actually causes infertility in these women. Also, when anovulation is prolonged, the endometrial tissue in the uterus can get very thick, resulting in heavy and/or irregular periods. The increase in androgens is also responsible for the excess hair growth and acne.
It also common for women with PCOS to have an insensitivity to insulin. This, many times, can predisposed them to have increased weight gain and obesity that places the patient at higher risk for diabetes and cardiovascular disease.
How can I get tested for PCOS?
There are no specific tests for PCOS, and the condition is essentially clinically diagnosed.
Your medical team will determine if there are any physical signs of excess androgens present, as well as evidence of ovulation problems by evaluating the length and regularity of your menstrual cycles.
Some testing may also reveal common features of the condition. For example, all Shady Grove Fertility patients undergo basic fertility testing including among others blood testing and ultrasound. The ultrasound can determine if the ovaries are enlarged and contain immature resting follicles, a prominent sign of PCOS. Blood testing can reveal or confirm elevated levels of androgen (male hormones). When making a diagnosis of PCOS, it is also important to rule-out other causes of ovulatory disorders, including thyroid dysfunction.
Once your physician has a complete picture and can make the diagnosis, he or she will work with you to create an individualized treatment plan.
Can diet and exercise help women with PCOS conceive?
“For overweight women with PCOS, weight loss is often the first step to increasing your chances of pregnancy,” Dr. Silva states. “The benefits of weight reduction include improved ovulatory function, improved chances of conception, a safer pregnancy for both the mother and baby, and—if needed—better response to fertility medications. Studies have shown that by losing just 5 percent of body weight, a woman can actually restore her menstrual cycle and ovulate on her own. Weight loss has also been shown to reduce other symptoms such as hair growth, acne, and balding.”
What medications are prescribed for PCOS?
For women with PCOS who are actively trying to conceive, it is advised to consult with your OB/GYN or a fertility specialist, since many women with PCOS are not ovulating. Your physician can prescribe medication to help stimulate ovulation.
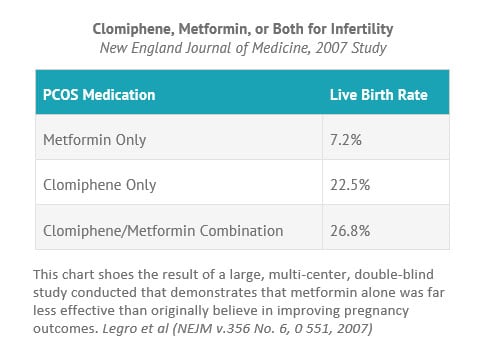
Oral fertility medications like clomiphene citrate (Clomid), which have been available for many decades, continue to be widely used to stimulate the development of an ovarian follicle containing an egg. Clomiphene citrate acts by blocking the action of estrogen in the brain (the hypothalamus and pituitary). As a result, there is an increased production of follicle-stimulating hormone (FSH), causing the development of one or more follicles. If ovulation is still irregular, additional medications can be prescribed. Metformin for example helps to make the body more sensitive to insulin, which can result in more regular ovulation.
What fertility treatments are available for PCOS?
Depending on the initial testing, a fertility specialist may recommend a patient to start ovulation induction medications (cited above) with timed intercourse or intrauterine insemination (IUI) that can be scheduled around the time of ovulation. For these treatments, it is important that the Fallopian tubes are open and the sperm counts are normal. The typical success rates with IUI is about 15 to 25 percent per cycle; a woman’s individual success rate with IUI is largely impacted by her age.
If ovulation induction with timed intercourse or IUI fail to achieve a pregnancy after a few attempts of this therapy, or if the patient also has other infertility factors such as blocked Fallopian tubes, her physician may recommend in vitro fertilization (IVF).
Do women with PCOS always have fertility problems?
Infertility is very common in women with PCOS. However, it is important to highlight that women with PCOS have a very good chance at conception. Patience and dedication may be necessary to allow an adequate amount of time for lifestyle modifications to enhance fertility naturally. When appropriate, being proactive about the initiation of medical therapy in these patients frequently results in a successful pregnancy. With the proper treatment, PCOS can be managed for the long-term and patients can live relatively symptom free.
To watch our On-Demand Webinar on PCOS, click here. During this free, on-demand event, viewers will learn about the symptoms of PCOS, the role they play when trying to conceive, and treatment options that are available to help women overcome their infertility caused by this condition.
Editor’s Note: This post was originally published in June 2016 and has been updated for accuracy and comprehensiveness as of September 2018.
To learn more about PCOS or to schedule an appointment with Dr. Silva, please contact our New Patient Center at 1-877-971-7755 or click here to complete this brief online form.