Shady Grove Fertility nurses Karen Calabrese, R.N. and Elizabeth Zapp, R.N. discuss some of the common questions patients ask about the 2-week wait.
The 2-week wait before you have your beta (pregnancy test) can seem like an eternity. Each day seems longer than the last, and the question “Am I pregnant?” goes through your mind hundreds of times a day. One becomes hyper-aware of your body’s every sensation. We all sympathize and wish there was some medical way to make the time shorter or easier for you. We’ve gathered some commonly asked questions, gave our nurse educators the opportunity to answer them, and shared them with you in hopes that it helps during this important time.
What is the 2-week wait?
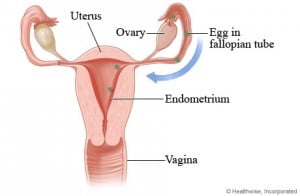
The 2-week wait is the period of time between the end of your fertility treatment cycle and beta hCG blood test—the test that determines whether or not you’re pregnant. It takes about 2 weeks from the time a fertilized egg implants in the uterine wall to start emitting enough of the hormone hCG (human chorionic gonadotropin) to be detected by a blood test. We sometimes call the test a “beta” because the test actually measures a beta chain portion of the hCG hormone molecule and is officially named a beta HCG test.
Can I take a home pregnancy test to see if I’m pregnant before my beta?
We recommend that you refrain from performing a home pregnancy test as they can render false results, either a false negative or false positive. A false positive result may be due to the fact that in many of our treatments, hCG, the same hormone that measures pregnancy, is given to “trigger” ovulation in many of our patients. Traces of the administered hCG can still be in your bloodstream and detectable by a test, even if implantation has not occurred.
A false negative might occur as a low level of hCG may be undetectable in a urine test despite a pregnancy starting, as home pregnancy tests are less sensitive than the blood hormone tests we use.
On average, about 2 weeks following your intrauterine insemination (IUI) or embryo transfer you will come back to our office for your pregnancy test. This test is done by blood draw and measures the hCG levels produced by the developing embryo. The most reliable pregnancy test is the blood test we perform in our offices.
What is happening to my body during the 2-week wait?
During this time, you may feel as if you are about to start your period. Your body has been through a lot and the medications you’re taking are designed to promote the optimal environment for pregnancy. You may experience some cramping, spotting or light bleeding, abdominal bloating, fatigue, and breast tenderness. While you may be slightly alarmed to experience some of these symptoms, they are normal and do not signify that you are or are not pregnant.
Please note, if after your treatment you feel excessive bloating, shortness of breath, chest pain, or lower abdominal pains, you may have ovarian hyperstimulation and should call your clinical team immediately.
Will I be taking medications during this time?
Yes. Most patients need to continue to take progesterone supplements in order to produce the same levels of hormones that would occur in early stages of pregnancy.
While most patients will supplement their progesterone via pill or vaginal insert, patients who are using donor egg or frozen embryos will use the injectable form of progesterone for their cycles.
Additionally, patients who undergo in vitro fertilization (IVF), donor egg, or frozen embryo transfers may also be prescribed estrogen supplements to help thicken and maintain the uterine lining.
Please do not stop taking these medications until you have been advised by your medical team to do so.
Can I continue my normal day-to-day activities during the 2-week wait?
We tell all of our patients to be cautious during their first 5 days after their treatment. We recommend that you refrain from strenuous physical activities as well as sexual activities during that time as they may cause uterine contractions that might impair the implantation process. There is also a greater risk during that time of ovarian issues arising since, for many patients, the ovaries are still slightly enlarged at that point.
After those first few days, you can start light aerobic activities such as yoga, swimming, moderate walking, and lightweight training on a stairmaster or elliptical trainer. Activities that can get your heart rate up, but are not demanding, are suggested rather than high-impact activities such as jogging or aerobics.
Do I need to adjust my diet during this time?
No special diet is required, but we recommend that you start making nutritional choices as if you’re already pregnant. This means eating well-balanced meals, no sushi or other raw or undercooked meats, avoiding high-mercury fish and soft cheeses, no alcohol, and continuing to take a preconception supplement.
Can I travel during the 2-week wait (or thereafter if pregnant)?
We prefer that patients avoid traveling for the first few days post-treatment, primarily so that you are close to our center for the examination should any problems develop. This also is true during and following the time of your pregnancy testing and ultrasound. Early pregnancy complications such as hyperstimulation, bleeding, or pain can occur and we would want you near your team for care. In addition, the rigors of travel, time zone changes, luggage, etc. leave you vulnerable to complications. Before you schedule travel during this period of time, check with your nurse and team to see what is advised.
If I am pregnant, how do you ‘count’ how far along we are?
As soon as it is determined that you are pregnant, we revert to the obstetrical counting/dating system. This is done to avoid using one set of dates from the time of an IUI or IVF versus another set of dates used by obstetricians. The OB doctors determine pregnancy dating to be from the last menstrual period, at least 2 weeks prior to ovulation. Obviously, we often know more about when ovulation may have occurred than they usually do, but for convention, we add 2 weeks to our dates to conform with the OB. As an example, if we know when ovulation was triggered and an IUI or IVF was performed, your beta might be 2 weeks thereafter. If it is positive, the OB would say you are 4 weeks pregnant, not 2, and therefore we do, too.
What are my next steps if I’m not pregnant?
If you are not pregnant, your nurse will advise you to stop your medications. You will have the opportunity to talk with your physician to review the past cycle and make a decision together about your next steps.
How long after a failed cycle can I do another cycle?
While your physician will determine the timing of a new cycle, it’s not always necessary to take time off between cycles unless otherwise directed. Many of our patients are able to begin their next treatment cycle immediately. For others, a cycle of rest may be recommended.
We know that these 2 weeks can be a very stressful time. Visit the SGF Facebook page if you’re looking for ways to help pass the time and get support from patients who understand what you are going through. If you have any questions, please don’t hesitate to call your nurse.
Reviewed and Updated: 2/21/2019