Medical contribution by Jason G. Bromer, MD, of Shady Grove Fertility’s Frederick, MD, office

Every year, most women find themselves back at their OB/GYN’s office for their annual gynecological exam. Prior to the visit with the doctor, you may fill out a questionnaire or a nurse may ask a barrage of personal questions, from your history with sexually-transmitted diseases (STDs) to the frequency you may drink and smoke. With the best intentions you will answer each of these questions, but sometimes, little white lies find their way into the answers given. For women trying to conceive, these little white lies may have a larger impact than realized. Read our top 5 little white lies that can make identifying a potential fertility problem harder.
Q: Are you a smoker? If yes, how much do you smoke?
A: Only when I drink or am really stressed, and only one or two cigarettes at a time.
Most people know that smoking can have an effect on their health. However, many don’t realize this includes their reproductive health. Compared to non-smokers, many smokers can experience up to a 54 percent higher chance that conception will take one year or longer. This delay in conception correlates with the daily quantity of cigarettes smoked. Smoking can also increase the rate of follicular depletion and reduce the levels of estrogen in the body.
Fertility treatment is also greatly impacted when the female partner smokes. Studies cite the following as side effects from smoking:
- decreased response to ovarian stimulation medications
- decreased number of eggs available for retrieval
- increased number of cancelled cycles
Smoking doesn’t only impact a woman’s fertility either. Smoking cigarettes can cause a decrease in the three main factors that determine a man’s sperm quality: sperm count, morphology (sperm shape), and motility (how sperm move). Studies have shown that damage is not necessarily permanent and may vary by the quantity and length of smoking history. A man’s fertility rate can completely return to normal within one year of quitting smoking.
Q: How many alcoholic beverages do you consume in one week?
A: I only have one or two glasses of wine with dinner.
Alcohol can impact a couple’s ability to conceive more than one might think. Studies have shown that women who consume a moderate amount of alcohol (up to 6 drinks per week) can experience a decrease in conception rates.
Like smoking, alcohol intake also impacts a man’s fertility. Men who consume more than 6 drinks per week are found to have a 14 percent lower chance of conceiving. Men who consume large quantities of alcoholic drinks (6 or more drinks) may have lowered testosterone levels and reduced sperm quality and quantity. Reducing the amount of alcohol consumed can quickly reverse the side effects caused to sperm.
Q: Have you ever been treated for an STD?
A: No…not that I can remember.
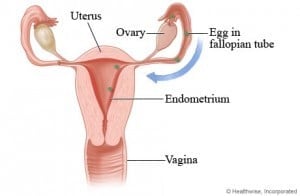
Sexually transmitted diseases (STDs)—even those that are successfully treated—can affect a woman’s fertility. STDs, especially chlamydia and gonorrhea, can cause inflammation and scar tissue that damage the fallopian tubes. Any damage to the fallopian tubes can make pregnancy much more difficult to achieve or prevent it all together. Patients with a history of STDs are also found to experience an increase in their risk of ectopic pregnancy—a pregnancy where the fertilized egg is stuck in the fallopian tube and must be removed.
A history of STDs does not necessarily mean that you will have infertility, but it’s worth getting checked out. There are simple tests, such as a hysterosalpingogram (HSG), that can evaluate the health of the fallopian tubes.
Q: Are your periods painful?
A: They aren’t anything I can’t handle.
Pain that is above and beyond the normal cramps associated with your period can be a sign of a endometriosis. With endometriosis, the uterine lining, called the endometrium, attaches and grows outside the uterus in the abdominal cavity. This endometrial tissue bleeds and causes inflammation and scarring which may block the fallopian tubes or interfere with their function. Endometriosis can also cause cysts in the ovaries that affect their ability to release eggs. With the right treatment, women with endometriosis have a good chance of getting pregnant.
Q: Are you still using contraception?
A: Sometimes…when we can remember.
Depending on your age, if conception hasn’t occurred within one year after stopping the use of any form of contraception, there could be a problem. Even if patients are not actively trying, the time passed still counts. Any change in contraception, from stopping birth control pills or the use of condoms during intercourse, should be discussed with your physician.
It is recommended that women under the age of 35 who have not conceived within one year, and women 35 and older who have not conceived within 6 months, speak with a fertility specialist. These recommendations do not mean that you will not conceive on your own, but it can be useful to get a check up and discuss if there might be any factors that may be impacting you or your partner’s fertility.
Living a healthy lifestyle is important when planning to conceive. If any of these little white lies sound familiar, work with your medical provider to make sure there aren’t any red flags you might be missing regarding your fertility. If you have been trying to conceive without success for over one year, schedule an appointment to get the answers you need and make sure you aren’t missing anything.
For more information or to schedule an appointment with one of our physicians, please speak with one of our friendly New Patient Liaisons by calling 888-971-7755.