
Medical contribution by Rebecca J. Chason, M.D.
Rebecca J. Chason, M.D., FACOG, is board certified in obstetrics and gynecology and reproductive endocrinology and infertility. Dr. Chason serves on the women’s health council at Anne Arundel Medical Center and is a member of the Academic Affairs Committee for the department of OB/GYN’s and will serve as core faculty for the developing residency programs. She sees patients at SGF’s Annapolis, Maryland office.
The leading cause of female infertility—affecting nearly 25 percent of infertile couples—is a problem with ovulation, also known as an ovulatory disorder. When a woman has problems with ovulation, she may ovulate irregularly, infrequently or even not at all. The most common cause of ovulation dysfunction is polycystic ovary syndrome (PCOS). But why does a problem with ovulation affect female fertility? How do you even know if you are ovulating? Most importantly of all, can these conditions be treated?
What is ovulation and how can I tell if I am ovulating?
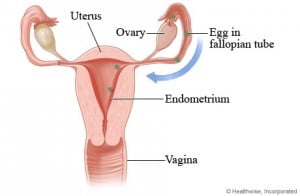
Ovulation is vitally important to becoming pregnant, as this is when the ovary releases an egg. During a woman’s monthly menstrual cycle, ovulation usually occurs around day 14, though the exact timing can vary among women or even from month to month. The day of ovulation and the 2 – 3 days just prior to ovulation are the best times to try to conceive. It’s during this time that the ovary will release the egg, which is then picked up by the Fallopian tube. Upon having intercourse, sperm will swim up the cervix, through the uterus, and into the Fallopian tube to reach the egg for fertilization.
One of the best signs of regular ovulation is a regular menstrual cycle. In addition, if you are ovulating, you may experience pelvic cramping or discomfort, a change in vaginal discharge, and/or a change in your basal body temperature (your body’s lowest temperature in a 24-hour period, often taken upon waking). An ovulation predictor kit can help detect ovulation by measuring luteinizing hormone (LH) in your urine. An LH surge (shown by a high level of LH in your urine) means that you will probably ovulate within the next 12 to 24 hours. If your cycle is irregular or if you rarely or never get a menstrual cycle, then you likely have a problem with ovulation. If you test your urine every day during your mid-cycle and do not detect an LH surge, you also may not be ovulating. In these situations it may be more difficult to determine when you are ovulating, making it harder to plan conception.
How are ovulatory disorders diagnosed?
Your menstrual history is very important to your physician when it comes to diagnosing possible ovulatory disorders. If you have regular cycles, it’s unlikely that you are not ovulating. But if your cycles are irregular, testing will be needed to diagnose whether or not there is a problem with ovulation. You may need one or more of the following tests:
- FSH blood level: This blood test measures the amount of follicle-stimulating hormone (FSH) in your blood. This helps measure ovarian reserve, meaning the number of eggs that you have in storage.
- Progesterone (P4) blood level: The P4 test measures the amount of progesterone in your blood to determine if ovulation has occurred.
- Ultrasound: An ultrasound is a scan that uses high-frequency sound waves to see if follicles in your ovaries are developing. Physicians also use ultrasound to evaluate ovarian function. For example, PCOS has a classic appearance on ultrasound.
What are the most common problems with ovulation and how can they be treated?
Anovulation: This is a disorder in which eggs do not develop properly or are not released from the follicles of the ovaries, signifying that ovulation is not occurring. Women with this disorder may not menstruate for several months. Others may menstruate even though they are not ovulating. While anovulation may result from PCOS, ovarian insufficiency (inadequate number of eggs), hormonal imbalances, eating disorders, and other medical disorders, it may also be unexplained.
Oligo-ovulation: This is a disorder in which ovulation doesn’t occur on a regular basis. The menstrual cycle may be longer than the normal cycle of 21 to 35 days.
- Course of Treatment: If you are not ovulating, your physician will likely prescribe a medication to stimulate ovulation depending on the underlying cause. If you decide to take medication to ovulate, your physician will monitor you carefully to see if and when you are ovulating. Monitoring usually involves ultrasounds and blood tests.
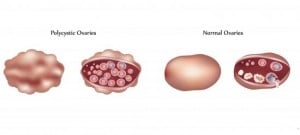
Polycystic Ovary Syndrome (PCOS): PCOS is a disorder in which the ovaries produce excessive amounts of male hormones and develop many small cysts. These hormonal imbalances can prevent ovulation. PCOS is associated with insulin resistance and obesity, abnormal hair growth on the face or body, and acne. PCOS is the most common form of ovulatory disorder.
Learn more in PCOS: The Big Picture
- Course of Treatment: For PCOS,
treatment will depend on your specific needs. Obesity may make the condition worse, so losing weight may help improve the hormonal imbalance. Regardless of weight as a factor, your physician will ultimately prescribe medication to stimulate ovulation. He or she may also prescribe other medications such as hormones or medications to treat women who have insulin resistance, in order to improve irregular or heavy periods and other symptoms.
Hypothalamic dysfunction: The two hormones responsible for stimulating ovulation occurrence each month–FSH and LH–are produced by the pituitary gland in a specific pattern during the menstrual cycle. Excess physical or emotional stress, a very high or low body weight, or a recent substantial weight gain or loss can disrupt this pattern and affect ovulation. The main sign of hypothalamic dysfunction is irregular or absent periods and often low estrogen levels.
- Course of Treatment: Hypothalamic dysfunction treatment will depend on the cause, but the most common treatment is medication to replace the FSH and LH hormones. Infrequently, a pituitary tumor may be present, in which case it can be treated with medication or surgery if necessary.
An excess of prolactin: The pituitary gland can produce excess amounts of prolactin (hyperprolactinemia), which reduces estrogen production and may cause infertility. This is usually a problem with the pituitary gland, but it can be related to medications you may be taking for another disease.
- Course of Treatment: Physicians typically prescribe medication to treat hyperprolactinemia. As with other conditions, though, there may be different causes (i.e., tumor, medication use) that lead to hyperprolactinemia, which would lend itself to different courses of treatment.
Though problems with ovulation can cause infertility, they are also very common, making them easier to treat. Shady Grove Fertility physicians know what to look for and are well versed in the types of medication and treatment options that can help overcome the problem and help you to become pregnant.
Editor’s Note: This blog was originally published in March 2015, and has been updated for accuracy and comprehensiveness as of January 2021.
To schedule a virtual consultation with an SGF physician, please call our New Patient Center at 1-888-761-1967 or submit this brief form.
References:
Staff, M. C. (2013) ‘Female infertility Causes.’ Mayo Clinic. Available at: http://www.mayoclinic.org/diseases-conditions/female-infertility/basics/causes/con-20033618 (Accessed: 5 March 2015).




