One of the most common questions infertile patients and couples ask is: will the treatment my physician recommends work? It is perhaps little known to many that the majority of infertility sub-specialists ask themselves a very similar question: what will the fertility treatment success rates be if I use different treatment options available to a specific patient or couple?
The Patient Predictor Using National Data
The Society for Assisted Reproductive Technology, or SART, recently published a Patient Predictor on their website. They base their predictions on information gathered from close to half a million assisted reproductive technology (ART) cycles (i.e., in vitro fertilization [IVF] and donor egg) from more than 320,000 women performed in the United States since 2006. To obtain a result, the patient must provide specific information, including:
- age, height, weight
- number of pregnancies and deliveries
- diagnosis of their infertility
- if she is seeking to conceive with her own eggs or with donated eggs
For patients interested in conceiving with their own eggs, the Patient Predictor produces the probability of achieving a live birth after one, two, or three ART treatment cycles. For those considering conceiving with donated eggs, the predictor will produce the probability of a live birth and compare it with the one that the patient would have if she were to use her own eggs.
Much like when predicting weather, the results from the Patient Predictor cannot be 100 percent accurate since such a perfect prediction must be based on many more parameters than the ones the patient is asked to provide. The resulting predictions are based on data from many patients with varying medical circumstances, not to mention varying protocols, laboratory techniques, and fertility treatment success rates that come with different infertility centers. Yet, in spite of the differences, the Patient Predictor gives a very good probability of live births within a relatively narrow scale of probabilities—for the majority of patients who fit the parameters required to make the calculations.
Shady Grove Fertility’s Unique Prediction Instrument
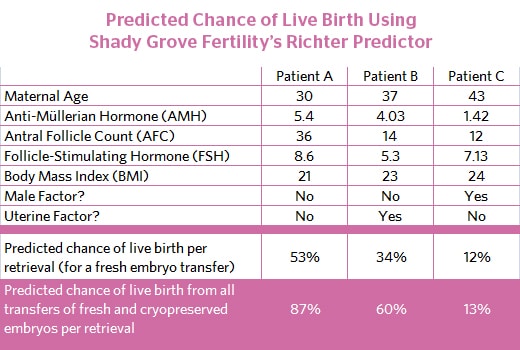
Many years ago, Shady Grove Fertility created its own predictor instrument, which is commonly known as the “Richter Predictor.” Named after Dr. Kevin Richter, Shady Grove Fertility’s Chief Statistician and Director of Research, the Richter Predictor is a more accurate predictor of success for SGF patients, specifically, not only because it leverages our own outcomes to determine probability, it also incorporates more clinically relevant parameters, such as:
- antral follicle count
- levels of anti-Müllerian hormone (AMH) and follicle-stimulating hormone (FSH)
- the presence or absence of uterine and sperm abnormalities
Shady Grove Fertility’s research team used a few different patient populations for various components of our prediction models. Altogether, we based our modeling on analysis of nearly 15,000 treatment cycles from nearly 10,000 patients since 2009. Unlike the SART Patient Predictor, Shady Grove Fertility’s model also includes predictions of the likelihood of having good quality surplus embryos available for vitrification and subsequent frozen embryo transfer (FET), and the potential increase in live birth rates per egg retrieval that could be achieved by using these vitrified embryos.
For many patients seeking infertility therapy, it is now possible to predict with a high degree of probability a live birth after treatment with ART. When using other low-tech treatments such as ovulation induction or intrauterine insemination (IUI), it is reasonable to estimate that the probability of a live birth after one treatment cycle is between a fourth to a fifth of that of an ART treatment cycle.
Richter Predictor Offers Tremendous Value and Insight to Patients Faced with Difficult Decisions
This tool provides outstanding value to our patients. Navigating through the many decisions patients have to make along their journey can be challenging. It’s our philosophy to not only inform our patients but to also take an active role and strong, encouraging voice to help them navigate better in a pretty uncertain place.
We’ve invested tremendous resources to help patients feel more confident in their decision making and increase their baseline knowledge. In fact, Shady Grove Fertility is one of the few fertility centers in the country to employ a full-time dedicated research staff, under the leadership of Dr. Richter. As part of our ongoing commitment to excellence in patient care, we continuously analyze our statistics and devote significant resources in order to stay at the forefront on research to make sure our success rates are the best they can be.
- Learn why SGF invests in research and how this benefits patients
- SGF gives back to the research community through its published works
We encourage our patients to have a conversation with their physician about their own success probability. No prediction method can offer a guarantee, and conditions—especially female age if she’s using her own eggs—affect outcomes significantly. The advantage to patients at Shady Grove Fertility is, because of our vast experience having performed more than 65,000 ART treatment cycles (fresh autologous IVF, donor egg, FET) since our practice began in 1991, we can fine tune and personalize the treatment protocol with amazing precision to maximize effectiveness. It is advisable for each fertility center to assess their success rates the way that Dr. Richter has done to more accurately estimate the probability of success.
If you would like to learn more about Shady Grove Fertility or are ready to schedule an appointment, please speak with one of our New Patient Liaisons at 877-971-7755.