One of the common misconceptions about fertility treatment is that multiples are standard and nearly inevitable. According to the CDC, the national rate of twins and higher order multiples (e.g. triplets or more) increased from 1998 to 2009. While historically twinning makes up about 2 percent of the live birth population, over this 21-year period the rate doubled. An important driver of this increase was the number of couples undergoing fertility treatment. Thankfully, and especially at SGF, rates of twins from fertility treatment are now declining due to improved IVF practices, such as blastocyst culture, preimplatation testing of embryos, and blastocyst vitrification, which enable highly successful single embryo transfer. For the story, “7 Things You Need to Know if You’re Pregnant with Twins,” US News talked to Dr. Kate Devine, Shady Grove Fertility’s Director of Clinical Research.
Looking back, why did couples experience more twins from fertility treatment?
Dr. Devine tells US News that until recently, fertility experts were more limited in their ability to examine the quality of embryos created during the in vitro fertilization (IVF) process. Determining which embryo(s) were best to transfer was done according to their rate of development and morphologic characteristics alone, and usually only over the course of the first two to three days of their development.
However, in recent years, improvement in embryo culture techniques have greatly improved our ability to observe and assess embryo growth and development for longer duration in the IVF lab. In addition, we now have the ability to do genetic testing on embryos to select a chromosomally normal embryo for transfer. If there are additional high-quality embryo(s), we can store them for the future. Prior to the advent of these technologies, it was difficult to select a single embryo with a high probability of implanting in a woman’s uterus and resulting in a healthy baby.
Therefore, physicians would typically transfer two and sometimes more than two embryos in hopes of successful implantation. And yes, multiple births were more common. Dr. Devine says, “The goal was to boost the woman’s chances of delivering a baby, since it wasn’t clear which embryos would make it.”
New Technology Results in Fewer Twins
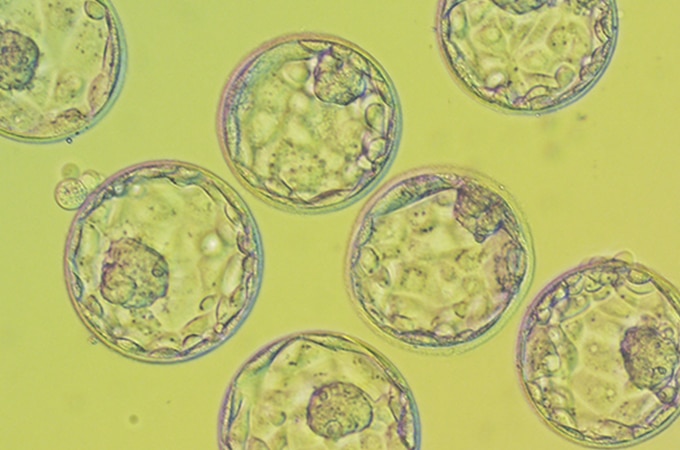
Today, technology allows embryologists and physicians to examine embryos much more carefully and select with confidence the one with the highest chance of implanting and resulting in a successful pregnancy. At Shady Grove Fertility we’ve long been proponents of elective single embryo transfer, or eSET. We observe all fertilized embryos until they reach the blastocyst stage. This is the stage when the embryo has differentiated into two parts: the inner cell mass, which is the potential fetus, and the trophectoderm, which has potential to become the placenta. It is also the stage at which the embryo implants in the uterus in both natural and IVF pregnancies. By combining blastocyst culture with single embryo transfer, we have drastically decreased the number of multiple pregnancies, while maintaining excellent IVF success. And by increasing the proportion of singleton pregnancies, we dramatically decrease health risks to both baby and mother.
The assumption that fertility treatment means twins is no longer correct or close to it. Thankfully, due to improvements in technology, SGF’s standard of care has changed to singleton pregnancies, enabling “one healthy baby at a time.” We are now better able to offer the best care for our patients leaving them with healthier choices for not only themselves, but for their baby and future children.
To learn more or to schedule an appointment with an SGF physician, please call our New Patient Center at 1-877-971-7755 or fill out this brief form.
Editor’s Note: This blog was originally published in Feb 2017, but has been updated as of July 2019.









.jpg) Jessica had a very successful egg retrieval, with 29 eggs retrieved. Because the couple had had a low sperm count on some of their previous cycles, the laboratory used
Jessica had a very successful egg retrieval, with 29 eggs retrieved. Because the couple had had a low sperm count on some of their previous cycles, the laboratory used  Jessica had used the Shady Grove Fertility Facebook page throughout her fertility treatment to get support from the community of patients who are active there. Now, she’s also using the Shady Grove Fertility Graduates Facebook page to talk to other women who became moms through fertility treatment. “I think all new moms want to talk to other moms,” she says, “but to be able to talk to moms who also went through IVF is really special. They give me a lot of great advice.”
Jessica had used the Shady Grove Fertility Facebook page throughout her fertility treatment to get support from the community of patients who are active there. Now, she’s also using the Shady Grove Fertility Graduates Facebook page to talk to other women who became moms through fertility treatment. “I think all new moms want to talk to other moms,” she says, “but to be able to talk to moms who also went through IVF is really special. They give me a lot of great advice.”